
 in young adults")
1 Introduction
The term positive mental health, first designated by Marie Jahoda in her report, emphasizes the significance of promotion in modern societies and the dynamic life cycle of people (1). This perspective underscores the importance of maintaining health and fostering positive aspects of one’s life.
Positive mental health is conceptualized as the mental health of healthy people, achieved through the optimization of general well-being for optimal functioning of each human being across the life cycle, which is not a static state but a dynamic process (2). Furthermore, positive mental health is a compelling protective element against mental disorders (3).
Promotion brings health gains to societies, and evidence suggests that positive mental health acts as key resilience factor against suicide (4). Additionally, positive mental health serves as a protective factor that can reduce the risks of addictive excessive social media use (5) and is a well-known protective factor against psychological distress and anxiety symptoms (6).
Mental health problems are among the most significant causes of illness worldwide (7). Adolescence, in particular, is a critical period where mental health disorders become notably pronounced. Many studies indicate a rising prevalence of mental health problems among adolescents across various countries (8).
In Portugal, mental and behavioral disorders constitute 11.8% of the overall burden of disease, surpassing oncological diseases (10.4%) and trailing only behind cerebrovascular diseases (13.7%) (9). These statistics are alarming, highlighting the need to address the 89.2% of the Portuguese population without mental illness to strengthen their resistance and mental well-being (2).
In 2022, the prevalence of positive mental health among different university Portuguese students was 67.8% for a high level of PMH, 31.6% for a medium level of PMH, and 0.6% for a low level of PMH (10). Another study carried out in 2017, revealed that university students were mainly at the moderate level (67.7%) of PMH, 16.6% at the low level, and 15.7% at the high level (11).
These findings align with other recent studies demonstrating good levels of positive mental health (12–14) despite the current reality.
Consequently, the first step is to use validated psychometric instruments tailored to the population under study as a means of investing in prevention. Secondly, it is deemed important to simplify the available psychometric instruments facilitating their use.
The Positive Mental Health Questionnaire (PMHQ) is a self-administered questionnaire with 39 items, originally developed in Spanish (15) and validated for the Portuguese population (16). The items vas distributed into the six factors of the Multifactorial Model of Positive Mental Health. The six factors include Personal Satisfaction (F1) referring to satisfaction with oneself (self-concept/self-esteem), with personal life and future prospects; Prosocial Attitude (F2), including the person’s sensitivity to one’s social environment, the attitude and desire to support others, and the acceptance of others and differentiating social facts; Self-control (F3) including the person’s ability to deal with stress and conflict situations, emotional balance and tolerance to frustration, anxiety and stress; Autonomy (F4) comprising the person’s ability to make decisions by applying personal criteria, self-regulating of self-behavior and maintaining a good level of personal safety; Problem Solving and Self-Actualisation (F5) referring to the person’s ability to make decisions and solve the problems that life entails and the ability to adapt to changes, developing a flexible attitude and continuous personal growth; and Interpersonal Relationship Skills (F6) including the person’s ability to communicate and establish harmonious interpersonal relationships with the surrounding environment and the ability to communicate feelings and give and receive affection (15, 17, 18).
In the PMHQ, values between 39 (minimum value) and 156 (maximum value) can be obtained, and the higher the value obtained, the greater the global level of positive Mental Health. Thus, different global levels of Positive Mental Health can be categorized: low Level or Languishing for scores between 39 and 78, intermediate Level for scores between 79 and 117, and high Level or Flourishing for scores between 118 and 156. The PMHQ allows for obtaining global and factor scores. Respondents are asked to answer based on the frequency that best characterizes their case, choosing from options between “Always or almost always,” “Most of the time,” “Sometimes,” and “Rarely or never.” Of these 39 items, 19 are formulated positively, and 20 items are formulated negatively. The responses presented in a Likert-type scale will produce different scores or values (2).
Therefore, this study sought to develop and validate the Positive Mental Health Questionnaire Short-Form (PMHQ-SF), an instrument intended to assess positive mental health in adults based on the previously validated Positive Mental Health Questionnaire – PMHQ.
2 Methods
2.1 Participants
The sample comprised Portuguese university students from 19 different institutions across the country and different areas of training, with a predominance of nursing students (54.7%). Initially, 3,647 participants were involved, but 110 were excluded because due to having at least one missing response in the Positive Mental Health Questionnaire (PMHQ), and ab additional 15 were excluded for failing to provide gender information. The final sample of 3,522 participants was randomly split into two groups: a calibration sample and a validation sample.
2.2 Measures
2.2.1 Positive mental health questionnaire
The scale was initially developed by Lluch-Canut with 39 items loaded into six factors: F1-Personal Satisfaction (items 4, 6, 7, 12, 14, 31, 38, 39), F2-Prossocial Attitude (items 1, 3, 23, 25, 37), F3-Self-Control (items 2, 5, 21, 22, 26), F4-Autonomy (items 10, 13, 19, 33, 34), F5-Problem Solving and Self-Realization (15, 16, 17, 27, 28, 29, 32, 35, 36), and F6-Interpersonnal Relationship Skills (items 8, 9, 11, 18, 20, 24, 30). The score ranges from 39 to 156. This scale shows good psychometric properties, with only Factor 2 presenting a lower Cronbach’s alpha (0.60) (15, 17).
The factorial structure of the scale was examined in a sample of Portuguese students (16), revealing good psychometric properties.
2.3 Analysis
Statistics analyses were conducted utilizing SPSS and R. One sample (N = 1,768) underwent exploratory factor analysis (EFA), and the other sample (N = 1,679) was subjected to confirmatory factor analysis (CFA). The selection criteria based on factor loadings in the EFA and CFA, with the highest chosen items. Oblimin rotation was applied for in EFA due to a correlation between factors suggested in previous studies. The factoring method selected was the principal factor solution, considering higher levels of kurtosis observed in some items. Multivariate analysis was conducted using three strategies: Mardia’s Test, Henze-Zirkler, and Royston.
An exploratory factor analysis (EFA) was conducted on the underlying structure of the measured positive mental health measured and subsequently, performed a confirmatory factor analysis (CFA). Measurement invariance was accessed by comparing models with increasing constraints to determine the degree of equivalence. In the configural model, the equivalence of structure without constraints was accessed; in metric invariance, loadings were constrained; in scalar invariance, the intercepts were compared; and for strict invariance, the model residuals were examined. A significant chi-square difference when comparing models indicated a lack of measurement invariance and a difference of CFI higher than-0.01 and RMSEA of 0.01 (19). The average variance extracted (AVE) was used to test convergent validity between constructs, with values above 0.70 considered very good and values below 0.50 indicating the difficulty in separating variance due to the construct itself and the one from measurement error (20).
3 Results
All variables exhibited acceptable skewness and kurtosis values, with item 3 presenting the highest kurtosis value in both the calibration and validation samples, namely 8.49 and 8.07, respectively, and skewness of -2.82 and -2.76, respectively (Table 1).
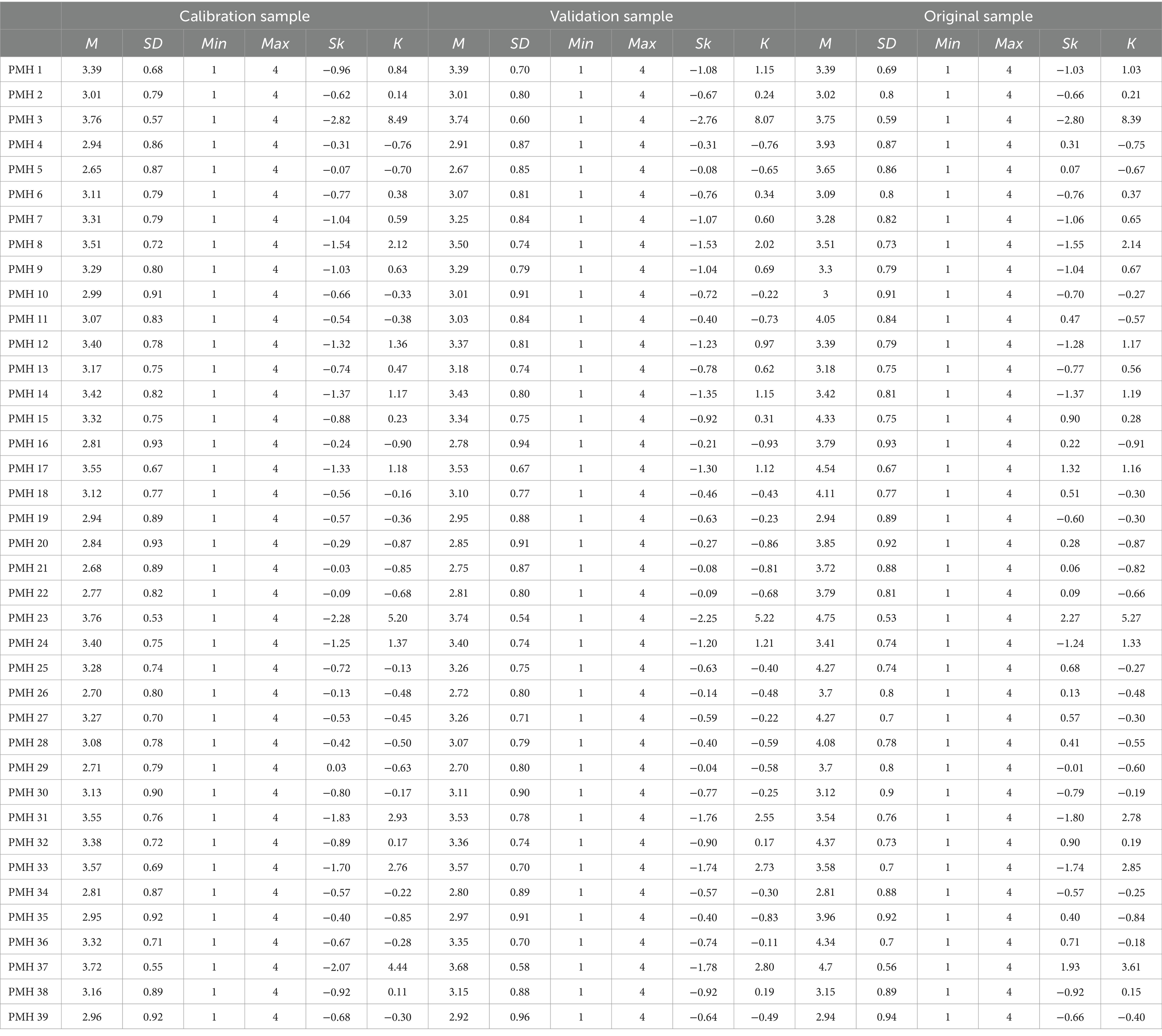
Table 1. Descriptive statistics for the validation and calibration sample.
Mardia’s test showed a violation of normality in both kurtosis and skewness (p < 0.001 for both). The chi-square test showed no differences between the calibration and validation in the distribution of gender and age. For this reason, principal axis factoring was applied for exploratory factor analysis and robust maximum likelihood was conducted for confirmatory analysis. The loadings of each item in the exploratory factor analysis are detailed in Table 2, with the items retained in the short form being highlighted.
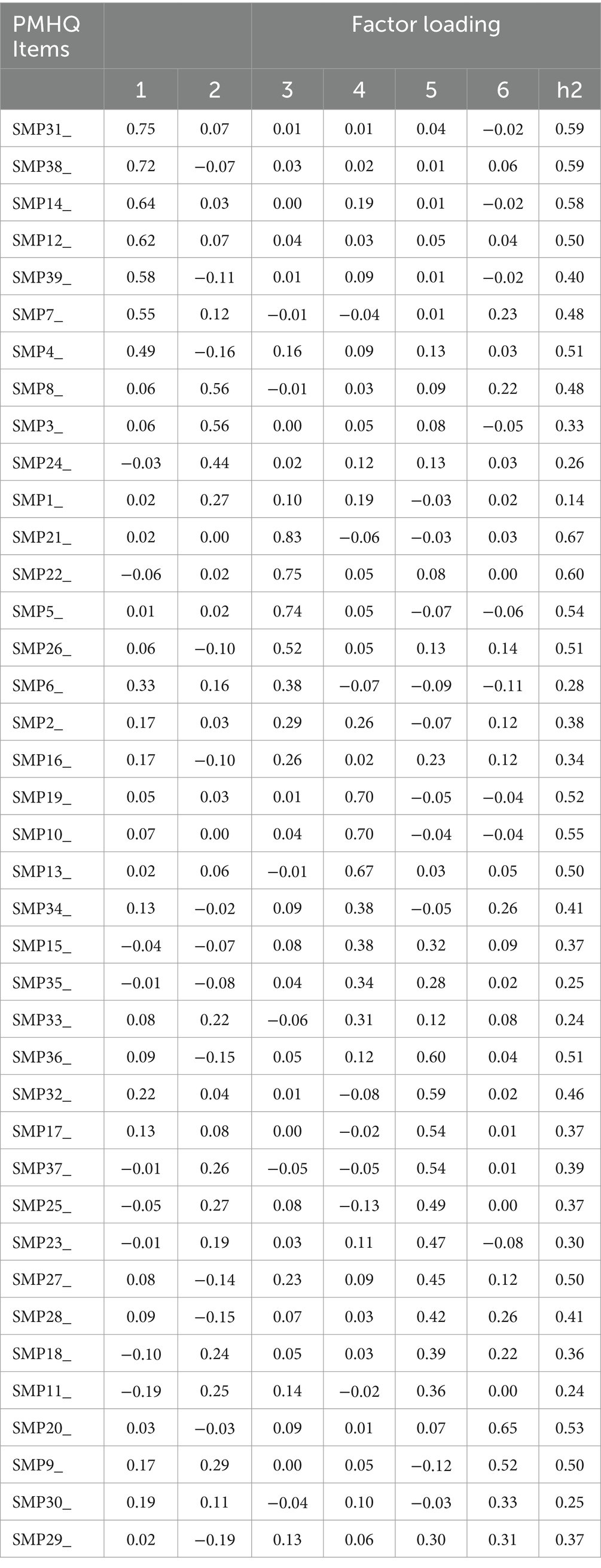
Table 2. Factor loadings for the exploratory factor analysis.
Only three items were selected for the short form, guided by the criteria of having the highest loadings in both EFA and CFA.
When the results of these two methods diverged, a model with both solutions was computed to identify the best fit. For factors F1, F3, and F4, the three items with higher loadings converging between EFA and CFA were selected for the short scale. For factor F1, items 14, 31, and 38 were retained; for factor F3, items 5, 21, and 22; and for factor F4, items 10, 13, and 19. Regarding factors F5 and F6, the two methods (e.g., EFA and CFA) produced different results, with only two of the three highest loading items being the same. For factor F5, the best items presented by the EFA were, in descending order of their factor loadings, items 32, 36, and 17. The CFA also showed items 32 and 26 to be amongst the highest loading but presented question 27 as the highest loading. When included in a short-form model tested by a CFA, 17 produced a better overall fit and was preferred to 27. Regarding factor F6, items 20 and 9 were identified in two of the highest loadings in both the EFA and CFA but for the other item to be retained, EFA had item 30 and CFA item 18. Again, the two items were included in a CFA of the final model, and item 30 exhibited a better fit. For factor F2, the CFA had items 23, 25, and 37 with the three highest loadings whereas, in EFA, only two of the four items were from the original factor (items 1 and 3).
In alignment with existing literature, it was decided to retain the items suggested by the CFA. Using a sample of Spanish university students, Roldan-Merino (21) verified that items 23, 25, and 37 had the highest loading when subjected to a CFA.
After comparing the results of both EFA and CFA, the final short scale was refined to include 18 items, with three items attributed to each factor (Table 2). To access the psychometric properties of the short scale, a CFA was conducted demonstrating a good fit, χ2 (120) = 580, p < 0.001, N = 1761, CFI = 0.97, TLI = 0.93, SRMR = 0.048, RMSEA = 0.045, p = 0.94, 90% CI [0.041, 0.049]. Reliability was tested using Cronbach’s alpha and MacDonald’s Omega, yielding acceptable results for each factor (a value higher than 0.60 was considered acceptable). The most problematic factor (Factor 2) exhibited the lowest reliability (0.60). The AVE values (Table 3) indicated convergent validity only for factors 1, 3, and 4.
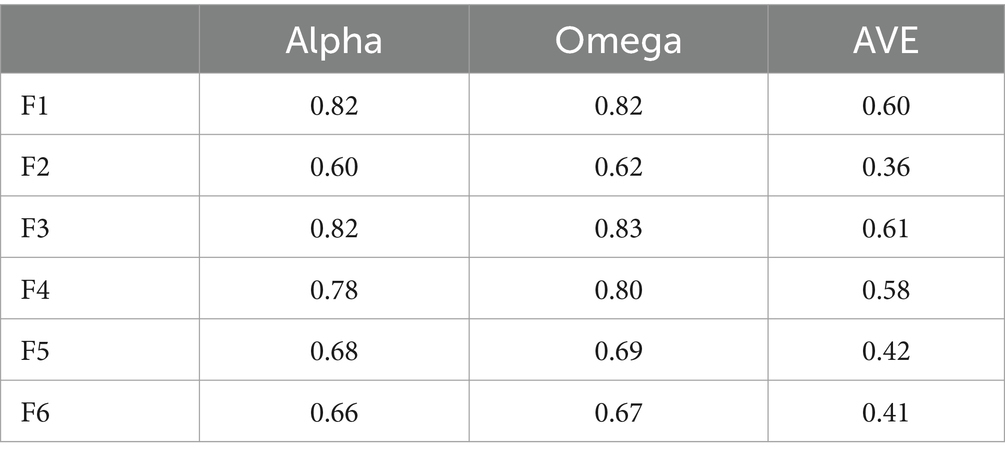
Table 3. Reliability.
The invariance analysis revealed metric invariance based on the chi-square criteria, with the CFI and RMSEA difference criteria supporting full invariance.
An additional analysis was conducted to evaluate the correlation between the composite factor scores in the full and proposed short form of the PMHQ-The results displayed very high correlations for all six factors and the total score of the scale, as presented in Table 4.
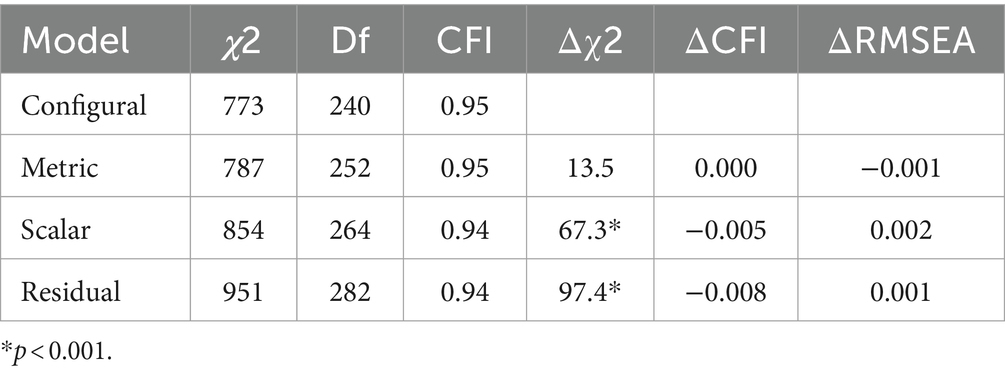
Table 4. PMHQ short form invariance.
Finally, cut-off points for the short form were examined by establishing three categories (e.g., low, average, and high total PMH scores) based on a standard deviation criterion of 1 SD. Specifically, 530 participants were identified with low positive mental health scores (M = 48.83), 2,445 participants exhibited average scores (M = 56.56), and 547 participants revealed high positive mental health scores (M = 64.29).
4 Discussion
This study aimed to create a short-form version of the PMHQ (Supplementary Appendix I). Overall, the psychometric properties of this short version yielded good results. The overall reliability of the PMHQ-SF18 is 0.92, with a factor ranging from 0.60 to 0.82. There are many instruments to measure well-being or mental health (22), but only fewer addressing a specific area of mental health – positive mental health.
Concerning the internal consistency of the PMHQ-SF18, these study findings for the global scale demonstrated good reliability (0.92). The Global Cronbach’s alpha value identified in this study is slightly higher compared to that reported by Almubaddel (23) in Saudi Arabia (0.86), by Hasan et al. (24), in Bangladesh (0.85), by Naghavi et al. (25), in Persia (0.90), and slightly lower than that found by Lukat et al. (26) in a German sample (0.93), and by Yilmaz and Eldeleklioğlu (27) in Turkey, where scales are based on other theoretical models.
Notably, factor F2 (Prosocial Attitude) exhibited reliability issues. However, this finding aligns with other studies, where this factor consistently displayed the lowest Cronbach’s alpha (Table 5). Thus, the short version demonstrates similar levels of reliability and validity when compared to the extended version.
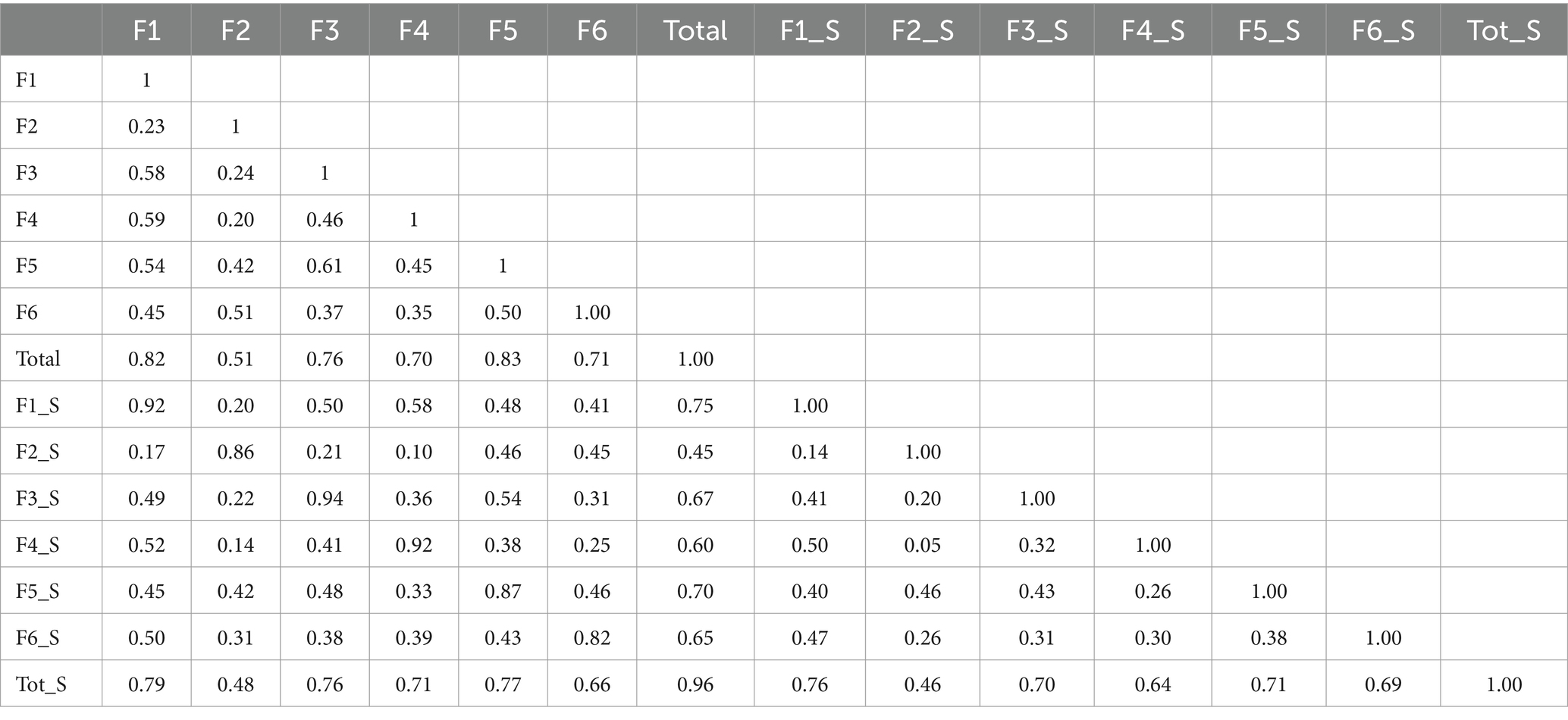
Table 5. Correlation matrix for the original and short form’s factors.
Moreover, the study by Sequeira et al. (16) involving Portuguese university students observed the same distribution of items originally from factor F2, with items 1 and 3 loading in the second factor, but items 23, 25, and 37 loading in factor F5. These results underscore that, since the original development of this questionnaire (17), this factor has revealed poor psychometric properties, and several studies advocate further evaluation in future research (17, 21). However, the significance of this conceptual factor and the results obtained in a validity analysis support retaining this factor (Table 6).
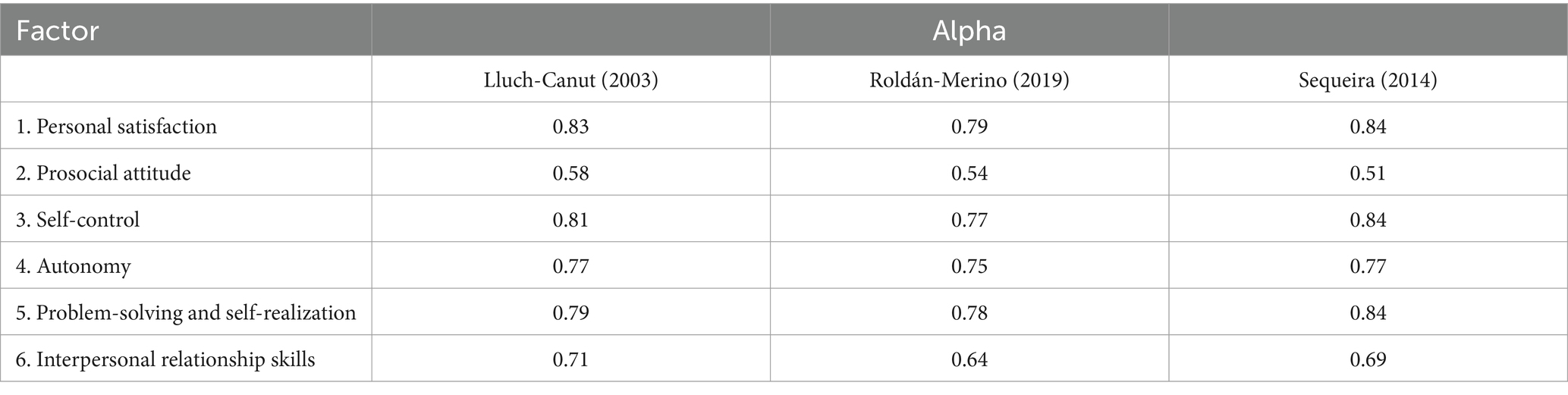
Table 6. PMHQ alpha studies.
The PMHQ-SF18 is a fast-filling instrument for measuring global positive mental Health, comprising six factors: Personal Satisfaction (F1), Prosocial Attitude (F2), Self-control (F3), Autonomy (F4), Problem-Solving and Self-Actualization (F5), and Interpersonal Relationship Skills (F6). It consists of 18 questions on a 4-level Likert frequency scale with scores ranging from 1 to 4.
For this analysis, the negative items must be inverted. A global PMHQ-SF18 score can be obtained from each of the six factors (minimum 3–12 maximum). The values of the global PMHQ-SF ranged between a minimum of 18 and a maximum of 72.
In this study, the issues found in factor F2 likely stemmed from poor cultural appropriation of the perception of helping others. This self-awareness of the need to set personal goals in promoting activities such as volunteering and unpaid functions in the community is not exactly rooted in the education priorities of the Portuguese population, which can affect the results of factor F2. Therefore, further insight and analysis of this issue are deemed pertinent.
This tool seems to overcome perceived barriers and facilitating factors to evaluate positive mental health, thereby addressing the imperative to support the development of effective mental health strategies (28). This is particularly crucial in the assessment phase and can pose distinct challenges across cultures. Another challenge to overcome was the short time for the application of the questionnaire (29), potentially interfering in the credibility of the answers. Therefore, this shortened tool proves to be quicker to administer.
4.1 Strengths and limitations
This study has several strengths. First, the substantial sample size enhances the interpretability of the results. Also, the outcomes hold significant relevance as the PMHQ-SF18 facilitates the assessment of mental health, thereby assisting health professionals across different settings in promoting mental health. Notwithstanding these results, certain limitations should be acknowledged. While these study results may be generalizable to young adult university students sharing similar socio-demographic characteristics, they may not to extend to populations with less homogeneous characteristics. Although these findings may offer valuable insights into the characteristics of the general population, it is imperative to validate these assumptions through further research.
5 Conclusion
The PMHQ-SF18 showed good psychometric properties, with reliability and validity values similar to those of the original extended version of the PMHQ. For this reason, the PMHQ-SF18 an effective instrument for measuring positive mental health among university students. Although this study has successfully demonstrated the reliability and validity of the PMHQ-SF18, further research involving larger samples is needed to provide additional scientific evidence supporting this short version.
6 Relevance for clinical practice
These study findings have noteworthy implications to inform mental health professionals about the availability of a shortened version of the Positive Mental Health Questionnaire. This study encourages mental health nurses and other professionals to incorporate the assessment of positive mental health into their practice using validated psychometric instruments. This short version with 18 items enhances its suitability for clinical practice, making it more practical and easier to apply.
Moreover, the social relevance of this study lies in its contribution to the advancement of positive mental health assessment and promotion strategies, particularly among young university adults. By providing a reliable and practical tool for assessing positive mental health, this study holds the potential to inform interventions that enhance the well-being and resilience of young adults, ultimately contributing to healthier and more supportive communities. The validation of a shorter version of the Positive Mental Health Questionnaire (PMHQ) among Portuguese university students fosters mental health promotion by offering a reliable and practical tool for assessing positive mental health. This study enhances early detection and intervention strategies by providing a culturally sensitive instrument that is accessible and feasible for young adults.
Data availability statement
The datasets presented in this article are not readily available because the data that served as the basis for the article is on an institutional basis from the Porto Superior School of Nursing. Data may be requested through a formal request as per data protection regulations. Requests to access the datasets should be directed to [email protected].
Ethics statement
This study was authorized by the Ethics Committee of the Porto Higher School of Nursing (2023_1945) and the participants provided written informed consent to participate in this study.
Author contributions
CS: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. JC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing. JR-M: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AM-P: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. ST: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. BD: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. PC: Data curation, Formal analysis, Methodology, Software, Writing – review & editing. MP-L: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. ML-C: Conceptualization, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This article was supported by the National Funds through FCT – Fundação para a Ciência e a Tecnologia, I.P., within CINTESIS, R&D Unit (reference UIDB/4255/2020 and reference UIDP/4255/2020), and by the Portuguese Society of Mental Health Nursing (ASPESM).
Acknowledgments
The authors wish to acknowledge the professional translator Maria do Amparo Alves for the editing of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at:
References
1. Jahoda, M
. Current concepts of positive mental health. New York: Basic Books (1958).
Google Scholar
2. Teixeira, S, Sequeira, C, and Lluch, T. Programa de promoção de Saúde Mental Positiva para adultos (Mentis Plus+): manual de apoio. Porto: A Sociedade Portuguesa de Enfermagem de Saúde Mental (2020).
Google Scholar
3. World Health Organization
. Prevention of mental disorders – Effective interventions and policy options. Geneva: World Health Organization (2001).
Google Scholar
4. Teismann, T, Brailovskaia, J, and Margraf, J. Positive mental health, positive affect and suicide ideation. Int J Clin Health Psychol. (2019) 19:165–9. doi: 10.1016/j.ijchp.2019.02.003
PubMed Abstract | Crossref Full Text | Google Scholar
5. Brailovskaia, J, and Margraf, J. Positive mental health and mindfulness as protective factors against addictive social media use during the COVID-19 outbreak. PLoS One. (2022) 17:e0277631. doi: 10.1371/journal.pone.0277631
Crossref Full Text | Google Scholar
6. Truskauskaite-Kuneviciene, I, Kazlauskas, E, Ostreikaite-Jurevice, R, Brailovskaia, J, and Margraf, J. Positive mental health and adjustment following life-stressors among young adults. Curr Psychol. (2022) 41:1951–6. doi: 10.1007/s12144-020-00714-3
Crossref Full Text | Google Scholar
7. Simkiss, NJ, Gray, NS, Malone, G, Kemp, A, and Snowden, RJ. Improving mental health literacy in year 9 high school children across Wales: a protocol for a randomised control treatment trial (RCT) of a mental health literacy programme across an entire country. BMC Public Health. (2020) 20:1–8. doi: 10.1186/s12889-020-08736-z
Crossref Full Text | Google Scholar
8. Patalay, P, and Gage, SH. Changes in millennial adolescente mental health and health-related behaviors over 10 years: a population cohort comparison study. Int J Epidemiol. (2019) 48:1650–64. doi: 10.1093/ije/dyz006
Crossref Full Text | Google Scholar
10. Teixeira, S, Ferré-Grau, C, Canut, TL, Pires, R, Carvalho, JC, Ribeiro, I, et al. Positive mental health in university students and its relations with psychological vulnerability, mental health literacy, and sociodemographic characteristics: a descriptive correlational study. Int J Environ Res Public Health. (2022) 19:1–12. doi: 10.3390/ijerph19063185
Crossref Full Text | Google Scholar
11. Nogueira, MJ, and Sequeira, C. A saúde mental em estudantes do ensino superior. Relação com o género, nível socioeconómico e os comportamentos de saúde. Rev Port Enferm Saúde Mental. (2017):51–6. doi: 10.19131/rpesm.0167
Crossref Full Text | Google Scholar
12. Eriksson, C, Arnarsson, ÁM, Damsgaard, MT, Löfstedt, P, Potrebny, T, Suominen, S, et al. Towards enhancing research on adolescent positive mental health. Nordisk välfärdsforskning Nordic Welfare Res. (2019) 4:113–28. doi: 10.18261/issn.2464-4161-2019-02-08
Crossref Full Text | Google Scholar
13. Bjørnsen, HN, Espnes, GA, Eilertsen, MEB, Ringdal, R, and Moksne, UK. The relationship between positive mental health literacy and mental well-being among adolescents: implications for school health services. J Sch Nurs. (2019) 35:107–16. doi: 10.1177/1059840517732125
Crossref Full Text | Google Scholar
14. Emine, E, Neslihan, L, and Sefa, L. Evaluation of the positive mental health levels of the students of the faculty of sports sciences. Sci Mov Health. (2021) 21:32–5.
Google Scholar
16. Sequeira, C, Carvalho, J, Sampaio, F, Sá, L, Lluch-Canut, T, and Roldán-Merino, J. Avaliação das propriedades psicométricas do questionário de saúde mental positiva em estudantes portugueses do ensino superior. Rev Enferm Saúde Mental. (2014) 11:45–53.
Google Scholar
17. Lluch, MT
. Construcción y análisis psicométrico de un cuestionario para evaluar la salud mental positiva. Psicol Conduct. (2003) 11:61–78.
Google Scholar
18. Lluch, MT
. Concepto de salud mental positiva: Factores relacionados In: J Fornes and J Gómez, editors. Recursos y programas para la salud mental. Enfermería psicosocial II. Madrid: Fuden (2008). 37–69.
Google Scholar
19. Putnick, D, and Bornstein, M. Measurement invariance conventions and reporting: the state of the art and future directions for psychological research. Dev Rev. (2016) 41:71–90. doi: 10.1016/j.dr.2016.06.004
Crossref Full Text | Google Scholar
20. Fornell, C, and Larcker, DF. Evaluating structural equation models with unobservable variables and measurement error. J Mark Res. (1981) 18:39–50. doi: 10.2307/3151312
Crossref Full Text | Google Scholar
21. Roldán-Merino, J, Lluch-Canut, MT, Casas, I, Sanromà-Ortíz, M, Ferré-Grau, C, Sequeira, C, et al. Reliability and validity of the positive mental health questionnaire in a sample of Spanish university students. J Psychiatr Ment Health Nurs. (2017) 24:123–33. doi: 10.1111/jpm.12358
Crossref Full Text | Google Scholar
22. Lindert, J, Bain, PA, Kubzansky, LD, and Stein, C. Well-being measurement and the WHO health policy health 2010: systematic review of measurement scales. Eur J Pub Health. (2015) 25:731–40. doi: 10.1093/eurpub/cku193
PubMed Abstract | Crossref Full Text | Google Scholar
23. Almubaddel, A
. Psychometric properties of a Saudi Arabian version of the positive mental health (PMH) scale. Psicologia. (2022) 35:2–9. doi: 10.1186/s41155-022-00232-0
Crossref Full Text | Google Scholar
24. Hasan, T, Hasan, MM, Perven, A, and Khan, MHA. Validation and psychometric properties of the Bangla version of positive mental health scale (PMH-scale). Heliyon. (2023) 9:e14663. doi: 10.1016/j.heliyon.2023.e14663
PubMed Abstract | Crossref Full Text | Google Scholar
25. Naghavi, A, Teismann, T, Asgari, Z, Eizadifard, R, and Brailovskaia, J. Validation of the Persian version of the positive mental health scale. BMC Psychiatry. (2021) 21:472. doi: 10.1186/s12888-021-03487-6
Crossref Full Text | Google Scholar
26. Lukat, J, Margraf, J, Lutz, R, van der Veld, WM, and Becker, ES. Psychometric properties of the positive mental health scale (PMH-scale). BMC. Psychology. (2016) 4:8. doi: 10.1186/s40359-016-0111-x
Crossref Full Text | Google Scholar
27. Yilmaz Akbaba, A, and Eldeleklioğlu, J. Adaptation of positive mental health scale into Turkish: a validity and reliability study. J Family Counsel Educ. (2019) 4:44–54. doi: 10.32568/jfce.569976
Crossref Full Text | Google Scholar
28. Robertson, H
. Perceived barriers and facilitating factors to positive mental health and engagement with support Services for Young Offenders – a systematic literature review. Educ Child Psychol. (2022) 39:56–85. doi: 10.53841/bpsecp.2022.39.2.56
Crossref Full Text | Google Scholar
29. Vaingankar, J, Abdin, E, van Dam, RM, Chong, SA, Tan, LWL, Sambasivam, R, et al. Development and validation of the rapid positive mental health instrument (R-PMHI) for measuring mental health outcomes in the population. BMC Public Health. (2020) 20:471–12. doi: 10.1186/s12889-020-08569-w
PubMed Abstract | Crossref Full Text | Google Scholar
link






