

Study selection
The study selection process is shown in Figure 1. After removing duplicates (k=1138 hits), two independent researchers screened titles and abstracts of the remaining k=1316 hits (agreement rate: 0,92%, interrater reliability Cohen`s Kappa = 0,43); k=1225 hits were excluded. The full texts of the remaining 89 publications were screened by two independent researchers to assess eligibility (agreement rate: 0,76%, interrater reliability Cohen`s Kappa = 0,5), 69 studies were excluded after full text screening (see Table 3). Consensus was always possible during the screening of title and abstract or full-text screening, so it was not necessary to ask independent third reviewers for their vote. All available abstracts were in English and no publication had to be excluded due to the language criterion.
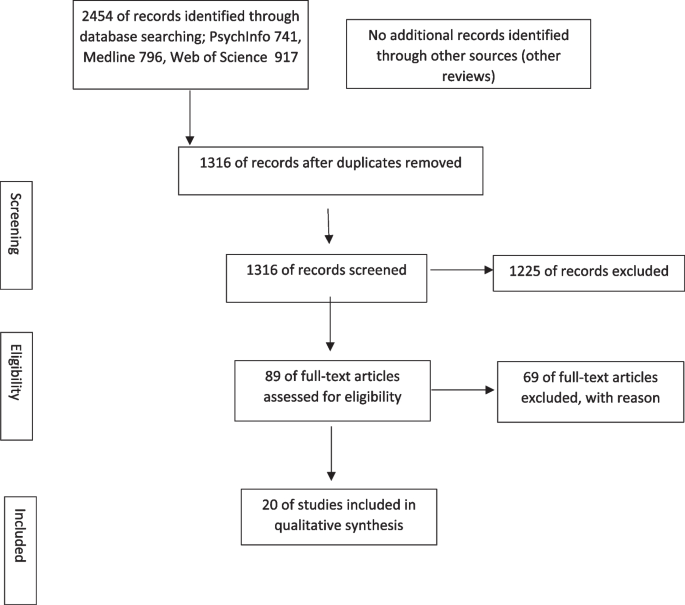
PRISMA-Flow-Diagram for the presentation of study selection process following Moher et al. (2009)
Populations investigated and background of investigators
Twenty studies fulfilled the inclusion criteria. Apart from Mateos-Fernándes et al. [31], which treated patients from the Sub Sahara region (Africa) and Poudel-Tandoukar et al. [32] investigating a Ukrainian refugee population (Europe), the patients in the remaining trials were all from Asia: five studies with refugees from Burma (Myanmar), four studies with refugees from Afghanistan/Iran, four with refugees from Syria, one mixed with Afghanistan/Iran and Syria, one study each with refugees from Sri Lanka, Cambodia and Bhutan. Seventeen interventions were culturally adaptions of an already existing therapy program or especially developed for refugees [32,33,34,35,36,37,38,39], the rest of the publications did not provide enough information in this regard. Apart from two first authors, the Indian author Vijayakumar and the Turkish author Acarturk, all first authors were from high income countries (6 from the USA, 5 from Germany, 2 from Netherlands, 4 from Australian, 1 from Spain). The host countries of the refugees were mainly high-income countries, in particular the USA and Europe (k = 10 studies). Three studies were conducted in Middle Income Countries [34, 40, 41] and two [33, 36] in low income countries (see Tables 4 and 5).
Only five trials had 100% of participants with clinical depression [36, 39, 42,43,44]. Northwood et al. [43], Wiechers et al. [39] and Cuijpers et al. [36] were quantitative parallel group-randomized trial studies, the others limited through a pre-post design not involving a control group. In ten studies, depression was a necessary inclusion criterion, but in six of these studies, depression was only one inclusion criterion alongside other mental disorders like PTSD [33, 34, 36, 40, 43,44,45,46]. Six studies used a diagnostic interview to identify depression [42, 43, 45, 47, 48], while others applied a cut-off score of a self-report measure to identify patients with potential clinical depression. Kinzie et al. [42] was the only study relying on a diagnosis by a health professional conducting a diagnostic interview based on DSM IV. For more details about the specificity of each intervention’s focus on depression, see Table 6.
Effectiveness of included trials by study design and treatment format
The content and dose intensity of the interventions varied. The intervention dose ranged from 5 [36, 37, 49] to > 40 sessions [41, 43, 48]. The highest number of sessions was reported in trials using multidisciplinary treatments, which were non-manualized and in a naturalistic setting. Seventeen interventions were manualized. CBT was the most studied intervention with four trials [34, 40, 46, 47]. Nine interventions were performed in an individual and ten in a group setting, with one being delivered digitally[36]. Treatment was mainly carried out by health professionals, but the Common Elements Treatment Approach [40], the Integrative Adapt Therapy [33, 34], the Contact and Safety Planning (CSAP) [41] and the interventions developed by the World Health Organisation (WHO Problem Management Plus (PM +) and Step by Step [35, 36, 38] were carried out by lay counsellors under supervision. In nine trials, the use of an interpreter was reported [31, 39, 41,42,43, 45, 48,49,50].
Studies involving a control condition
Nine studies used a control condition [34,35,36, 38,39,40,41, 43, 46]. Four were conducted in an individual setting, four in a group setting and one digitally. The sample sizes ranged from n = 24 [46] to n = 1755 [41], with the median of n = 322 participants.
Individual setting
Bolton et al. [40] examined the relative efficacy of a Common Elements Treatment Approach (CETA) compared to a waiting condition. CETA is a transdiagnostic treatment based on CBT, designed especially for delivery by non-professional providers in low-resource settings with few mental health professionals. It has a set of nine cross-cutting treatment components with decision-making rules and guidelines.
Problem Management Plus (PM +) was developed by the WHO as an intervention for underserviced communities and to be delivered by lay workers. PM + comprises 5 sessions: psychoeducation and stress management using diaphragmatic breathing (session 1), problem solving (session 2), behavioural activation by re-engaging with pleasant/task-oriented activities (session 3), accessing social support (session 4) and relapse prevention (session 5) [35]. De Graaf [35] compared PM + with a control group receiving care as usual which included all (mental) health services in the Netherlands. Additionally, PM + was delivered in a group setting in a trial by Acarturk et al. [38].
Northwood et al.[43] investigated the efficacy of the intensive psychotherapy and case management (IPCM) compared to a control group that received care as usual (CAU). CAU patients could be referred to a full range of behavioral health services by their primary care physician. IPCM is a behavioral health intervention consisting of psychotherapy and case management provided by refugee trauma specialists from the Centre for Victims of Torture (CVT) within two urban primary care clinics. The interventions were individually tailored and not manualized.
Vijayakumar et al. [41] compared two refugee camps in India, with one of the camps representing the passive control condition to the experimental condition called Contact and Safety Planning (CASP). The aim of the trial was to detect and reduce suicidal behavior among refugees, with depression representing a secondary focus. After a screening of all refugees in the camps, refugees with a high risk of committing suicide were observed by community volunteers who used safety planning cards. The community volunteers made periodic visits to provide emotional support to individuals who were depressed or suicidal. The safety planning card consisted of an individualized list of coping strategies containing names and contact numbers of persons in the individual`s immediate family, social circle and health services who could be contacted in a crisis [41].
Group setting
Kananian [46] compared Culturally Adapted Cognitive Behavioural Therapy plus Problem Solving (CA-CBT +) to a waitlist condition. CA-CBT + is based on the cultural adaptions of Cognitive Behavioural Therapy (CBT) by Hinton [51] and was adapted to the Afghan culture. The sessions covered the topics psychoeducation, emotional distancing and regulation techniques, mindfulness and relaxation techniques, anxiety, trauma recall and anger protocols, working with cognitions, somatic complaints and cultural syndromes. In contrast to the other studies with a control group design, which have a sufficient number of subjects (> 130 participants), Kananian et al. [46] included only 25 participants.
An RCT with care as usual as a control condition was conducted by Wiechers et al. [39] in Germany with refugees who were native-speakers of Arabic or Dari/Farsi and/or fluent in English or German. The intervention Empowerment group therapy for refugees (Empowerment) is based on cognitive behavioral therapy and comprises 16 sessions, each starting with a breathing exercise. Sessions 1–5 focus on psychoeducation and behavioral activation in the context of displacement. A culturally sensitive explanatory model is developed. Sessions 6–10 impart coping skills in dealing with migration-related acute stress, disturbed sleep, and somatic pain. Sessions 11–14 focus on emotion regulation strategies. In the final two sessions, information about further treatment options within the German mental health system is given.
Tay et al. [34] compared Integrative Adapt Therapy (IAT) to manualized CBT. Lay counsellors delivered IAT under supervision. The aim was to help refugees trace their emotional and behavioral problems to the underlying psychosocial disruptions. IAT is based on the Adaption and Development After Persecution and Trauma (ADAPT) model [52], which identifies five key psychosocial systems that support mental health in stable societies but are undermined by the refugee experience: safety/security, attachments, justice, role/identity disruptions, existential meaning. Seven treatment strategies (skills) were trained: psychoeducation, trauma narrative/modified exposure, problem solving, stress management, emotional regulation, cognitive reappraisal, meaning making [34].
Acarturk et al. [38] examined group gPM + for Syrian refugees in Türkiye against care as usual. The treatment consisted of 5 weekly group sessions, each of 2 h, delivered by non-specialists. For a description of the content of the sessions, see 3.2.1.1.
Digital intervention
The digital intervention Step-by-Step was based on behavioral activation, guided by nonspecialized helpers [36]. In five-sessions on an internet-connected device psychoeducation and training in behavioral activation were mediated through illustrated narratives. Therapeutic techniques such as stress management, a gratitude exercise, positive self-talk, strengthening social support, and relapse intervention were introduced. The narratives could be adapted to the user. The tool has a female and male version, each with two versions for different living situations (married with children or unmarried) and participants can choose the appearance of the character. Patients could use their phone or a computer in the camp during the trial. Cuijpers et al. [36] compared Step by Step with enhanced care as usual (ECAU). ECAU consisted of the first session of Step-by-Step, a basic psychoeducation, and a referral to evidence-based care, delivered through the app or website.
Summary of findings from controlled trials
Only the study by Vijayakumar et al. [41] showed no significant improvement in the symptoms of depression, however in this study the suicide rate improved significantly. Acarturk et al. [38] reported significant change only in the subgroup of those with probable baseline depression and not in the total sample. All other studies reported a significant reduction of depressive symptoms. It is notable that most of the randomized controlled trials reviewed here reported large treatment effects for reducing depressive symptoms (see Table 7). IAT was superior to CBT and specialized treatment was superior to care as usual. Apart from Tay et al. [34] the trials did not include credible control conditions, which hinders any conclusion about the efficacy of non-specific factors. CETA, Empowerment and the digital intervention Step-by-Step had high dropout rates (21%, 47% and 46%), indicating that while the interventions seems effective, they may not be well accepted. The studies varied in content and the extent to which various components were applied. The absence of treatment fidelity checks adds to the difficulty in disaggregating the specific components of effective treatment. This highlights the need for more investigation into treatment efficacy, the mechanisms of change, as well the acceptance of treatment methods amongst refugees before recommendations can be made.
Studies not involving a control condition
Eleven studies did not involve a control condition. Five were conducted in an individual setting and five in a group setting. The sample sizes ranged from n = 7 [47] to n = 144 [33] with the median of n = 29 participants.
Individual Setting
Kinzie et al. [42], Stammel et al. [48] and van Wyk et al. [50] studied multidisciplinary treatments in specialized centers. They offered culturally tailored psychotherapy, medication, counselling and social work. The interventions were diverse and patient-centered, not manualized, depending on the individual needs of the patient and on the capacities of the health professional. They treated the patients for about a year on a weekly or biweekly basis. Brakemeier et al. [45] offered Interpersonal Integrative Therapy for Refugees (IITF—abbreviated from the German term Interpersonelle Integrative Therapie für Flüchtlinge). The patients received 25 weekly sessions that focussed on modifying five treatment foci: role change, integration, interpersonal conflicts, grief, and isolation/loneliness. Pishyar et al. [37] reported on a small group of patients (n = 16) whom the author treated using the therapeutic de-reflection intervention [44]. De-reflection intervention is a logotherapy technique that aims to decrease negative self-observation by directing attention from problems and symptoms to meaningful values in the patient’s life, helping individuals to move toward self-transcendence. The therapy includes activity planning, multidimensional hygiene, a personal journey toward self-transcendence, managing negative attitudes and self-focused attention.
Group Setting
Berkson et al. [49] investigated the Cambodian Health Promotion Program (CHPP), a culturally tailored health education program for refugee survivors of torture, which uses handouts and videos for information transfer. Five key elements are a part of the training: 1. concept of health promotion and disease prevention, 2. nutrition, 3. physical activity, 4. stress, depression and sleep, 5. relationships. Kananian et al. [47] executed a pilot study for the CA-CBT therapy [46] but without the problem-solving sessions. Poudel-Tandukar et al. implemented an intervention called Social and Emotional Wellbeing (SEW) in two different populations. One trial was with Ukrainian and one trial with Bhutanese refugees in USA [37, 53]. It is a community based and culturally tailored multimodal intervention. Each session consists of health education, a problem-solving activity (60 min), breathing exercise and yoga (60 min). SEW has five modules: managing stress, strengthening communication skill, strengthening social networking, problem solving, creating a healthy family environment. Tay et al. [33] evaluated the previously described Integrative Adapt Therapy (see also 3.2.1.2) within a group setting (IAT-G) during the emergency phase of a mass humanitarian crisis amongst Rohingya refugees in Bangladesh. This group intervention with five to eight participants comprised seven sessions, each lasting 90 min. Each session focused on a psychosocial support system or pillar of the ADAPT model (see 3.2.1.2). After a reflection and sharing phase in each session, CBT strategies were introduced by lay workers to deal with feelings of stress related to the disruption of the ADAPT pillars. In addition, psychoeducation and skills were mediated. The Art Based Intervention (ABI) studied by Mateos-Fernándes et al. [31] represents a further form of intervention. ABI was developed for and evaluated by a group of irregular refugees and consists of drawing, dance, musical improvisation and relaxation.
Summary of findings from non-controlled trials
The studies were mostly of a pilot nature with a limited number of participants. Except for the pilot study by Kananian et al. [47], all studies showed a significant improvement of depressive symptoms from pre- to post- intervention. Kinzie et al. [42], van Wyk et al. [50] and in two trials Poudel-Tandukar et al. [37, 53] even achieved remission rates of above 30%. The trial by Kananian et al. [47] showed no significant change in the Patient Health Questionnaire (PHQ) but significant symptom reduction measured by the General Health Questionnaire (GHQ-28) subscale for depression. In a later trial by Kananian et al. [46] with more participants, the reduction in the PHQ values also became significant. Note, however, that the authors allowed additional medication. Confounding variables were hardly recorded, so that the significant mean changes between pre- and post-treatment are hardly meaningful. Nevertheless, the studies provide important information for the development of interventions. It seems that the use of psychotherapy at least does not lead to a worsening of symptoms. There is therefore no risk associated with the implementation of such interventions and they were mostly accepted by the refugees. Only the trials of Brakemeier et al. [45] and Kananian et al. [47] had high dropout rates (> 20%). For more details see Table 8.
Methodological quality assessment of included studies
The applied quality criteria can be found in Table 9. Acarturk et al. [38]was the only study with high quality ratings. Apart from the RCT by Vijayakumar et al. [41] and Wiechers et al. [39], which were rated low, the quality of all other RCTs (k = 6) was classified as moderate. Reasons for a moderate rating were often insufficient or inadequate information about the outcome data, for example high drop-out rates [36, 39, 40]. Non-randomized studies are already of poorer quality due to their study design. But even within their category, the identified trials scored poorly with k = 8 trials categorized as low quality. No study was of high quality and k = 3 were of medium quality [42, 45, 48]. For example, k = 7 trials categorized as low quality did not consider confounding variables (see Table 9).
link







