

Findings from systematic review
Study selection process
A total of 3,196 studies was identified in the initial database search. An additional three articles were identified through citation searching. After deduplication, 3,014 articles remained. A total of 2,874 articles was excluded based on screening titles and abstracts. Of the remaining 140 studies, 86 were excluded after the full-text review. The most common reasons for exclusion related to study design (non-RCT), the intervention lacking psychological components and/or not targeting a relevant outcome, or not providing sufficient information about the studied population (Fig. 1). Ultimately, 54 studies were eligible for inclusion in the systematic review [7, 18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70].
Study characteristics
The characteristics of the included studies on the efficacy of psychological interventions targeting overweight and obesity in school-aged children are demonstrated in Additional file 2. Most of the studies (41 out of 54 included studies) were published within the recent 10 years (as of 2023), indicating increasing focus on this topic as a global public health challenge.
Most studies (n = 31) were conducted in the US [18, 20, 22,23,24, 28, 30, 32, 34, 36,37,38, 40, 41, 43, 45,46,47,48,49, 51, 54, 55, 60, 61, 65, 66, 68,69,70], followed by Iran [19, 29, 57, 62], UK [33, 53, 63], Denmark [31, 35], the Netherlands [42, 58], China [39, 67], Israel [27, 52], Germany [7], Spain [21], Iceland [25], Turkey [26], Norway [44], Belgium [50], Switzerland [64], Australia [56], and Mexico [59].
Sample sizes ranged from 27 participants in a call-based intervention [32] to 549 in a community and clinic-based intervention [39]. Cognitive therapy alone or in combination with other behavioral methods was the most applied approach in the included studies [18,19,20,21,22, 27,28,29,30, 34, 36, 37, 42, 44, 48, 50, 55, 56, 58, 61, 64, 65, 68]. BMI z-score and BMI were the most frequently used outcome measures [18, 20, 21, 23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59, 61,62,63,64,65,66,67,68,69,70].
All studies applied multi-component psychological interventions based on either nutritional and/or physical activity programs for weight reduction. Quality of life (QL) [18, 19, 47, 54, 60, 63], dietary intakes [18,19,20, 23, 29, 39, 45, 48, 66], and physical activity (PA) [19,20,21, 23, 34, 39, 48, 63] were measured using a wide range of assessment tools.
Intervention duration ranged from 1.5 months in a day-camp and home setting intervention [31] to 36 months [20] (intervention setting was not provided by the researchers). Intervention sessions were variable (e.g., daily, or monthly basis). Follow-up time ranged from 2.5 months [31] to 24 months [27, 35]. In more than half of the studies (35/54), intervention groups were compared with control groups, while in the rest of the studies two or three intervention groups were compared. The reported interventions were implemented by people from a wide range of academic and professional backgrounds (e.g., school nurse, psychologist) and educational levels (e.g., master-level instructors, professional intervention delivery agent). Overall, most studies used professionals to implement the interventions, whereas in one study [51], intervention was delivered by using, an automated interactive voice response system (machine).
Type of psychological interventions
As illustrated in Additional file 2, different types of psychological interventions were applied and evaluated in the reviewed studies (e.g., cognitive behavioral, motivational interviewing).
Psychological intervention designs
Figure 2 summarizes different psychological intervention designs used in the included studies. Group-based interventions represented the most common intervention design. Most interventions targeted both children and their parents [18,19,20,21, 24,25,26,27, 30, 32, 35,36,37,38,39, 41, 43, 46, 48, 50, 51, 55, 57,58,59, 61, 62, 64, 66,67,68,69,70]. Individual designs were applied in five studies that focused on children or adolescents [23, 28, 33, 34, 54].
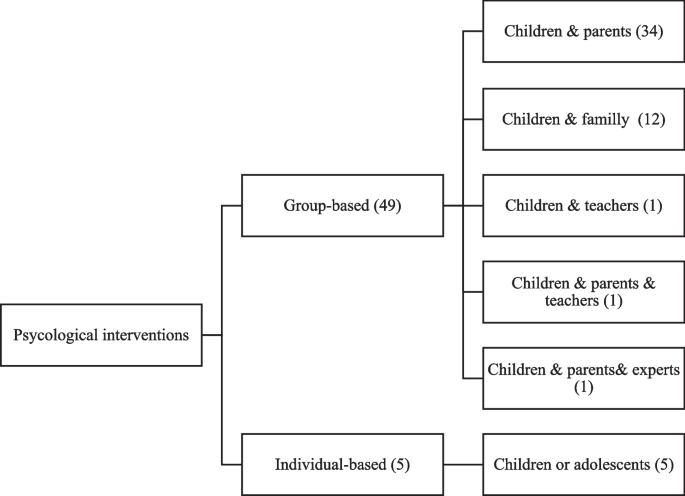
Psychological interventions designs targeting overweight, and obesity in school-aged children (based on studies included in systematic review)
Strengths and limitations of the intervention designs and methods
Table 1 illustrates strengths and limitations of different psychological designs adapted from [21, 58, 71,72,73,74,75,76,77,78,79,80,81,82] additionally with authors’ opinion. Furthermore, the following paragraph provide an overview on the main strengths and limitations of the most prominent psychological intervention methods- adapted from [83,84,85], additionally with authors’ opinion.
As the most frequent method in the reviewed studies, CBT covers a wide range of psychological aspects and social consequences of obesity from anxiety and loneliness to weight loss. It can also facilitate long-term weight-maintenance skills and improve a person’s self-esteem and -image. However, it also has limitation meaning that CBT alone will not work for everyone with obesity. So, it might be combined with other interventions like lifestyle changes to provide better results on obesity management.
MI alone, or in combination with CBT, also featured in the reviewed studies. MI has a strong theoretical foundation that emphasizes the importance for the individual to recognize and internalize why change is necessary and how change can be achieved. However, this highly individualized approach is also a limitation as implementation requires extensive tailoring to the target individual or group.
Findings from meta-analysis
Of the 54 included studies, 30 were eligible for inclusion in the meta-analysis [7, 18,19,20, 23, 24, 27,28,29,30, 33, 34, 36, 37, 39, 40, 44, 48, 50,51,52,53,54, 57,58,59,60,61, 65, 67]. Reasons for excluding 24 studies from further analysis were due to several issues (e.g., having unclear, insufficient, or missing data). The combined sample size of RCT studies included in the meta-analysis totaled 4093 school-aged children with overweight or obesity.
The pooled intervention effect is shown in Table 2. The intervention effect was statistically significant on all BMI measures (BMI and BMI z-score) (SMD: -0.59, 95% CI: -0.89, -0.20, I2 = 96.64), BMI z-score (SMD: -0.39, 95% CI: -0.69, -0.09, I2 = 88.60) and BMI (SMD: -0.79, 95% CI: -1.48, -0.09, I2 = 97.80). We also detected statistically significant intervention effects on fat mass (SMD: -0.96, 95% CI: -1.54, -0.38, I2 = 85.00), body fat (SMD: -0.81, 95% CI: -1.30, -0.33, I2 = 69.29), and diastolic blood pressure (SMD: -0.49, 95% CI: -0.83, -0.15, I2 = 41.80).
The pooled maintenance effect of intervention is shown in Table 3. Mean BMI and WC did not differ significantly between post-treatment and last follow-up measurement, indicating that initially lost weight is not regained during a subsequent follow-up period (maintenance effect).
Table 4 shows the results of sub-groups meta-analyses by type, duration, design, and intensity of psychological intervention, population age, and type of control group. In sub-group analyses the significant effect of psychological interventions on BMI was observed in studies conducted on children > 12 years old (SMD = -0.79, 95% CI: -1.57, -0.01), group-based interventions (SMD = -0.98, 95% CI: -1.80, -0.16), intervention of moderate intensity (SMD = -1.40, 95% CI: -2.56, -0.23), and interventions with a passive control group (SMD = -0.41, 95% CI: -0.79, -0.02). Moreover, the significant effect of psychological interventions on BMI z-score was observed in studies with very low (SMD = -0.88, 95% CI: -1.20, -0.56) or moderate intervention intensity (SMD = -0.96, 95% CI: -1.83, -0.10), or studies conducted with treatment-as-usual control group (SMD = -0.86, 95% CI: -1.04, -0.67). Significant effects on WC were observed in studies with low intervention intensity (SMD = -0.34, 95% CI: -0.59, -0.09) or studies conducted with passive control groups (SMD = -0.24, 95% CI: -0.44, -0.04).
MI and CBT—as effective psychological interventions—significantly reduced BMI z-score (generalized obesity) (SMD = -0.66, 95% CI: -1.15, -0.17) and WC (abdominal obesity) (SMD -0.53, 95% CI: -1.03, -0.04), respectively.
The highest pooled SMD in BMI z-score (SMD -0.96, 95% CI: -1.83, -0.10) was observed in interventions of moderate intensity.
Figure 3 shows forest plot of intervention effects on BMI measures in our target population.

Forest plot of psychological intervention effect on BMI measures in school-aged children with overweight and obesity
Meta-regression
Sufficient data were available to perform a meta-regression analysis of intervention effect on BMI z-score, BMI, and WC by intervention type, duration, design, and intensity, age, and type of control group. Meta-regression of BMI-z score showed that age (coefficient: -0.77, SE: 0.22; p < 0.100), intervention intensity (coefficient: 0.18, SE: 0.08; p < 0.100), and type of control group (coefficient: -0.42, SE: 0.14; p < 0.100) contributed to the heterogeneity. No sources of heterogeneity were found for BMI and WC.
Quality of the studies
The kappa statistic for agreement of quality assessment was 0.90. The quality assessment of the included studies is presented in Additional file 2. Of 54 included studies, 22 (41%) were rated as low risk of bias. While eight studies were rated as high risk of bias. For the rest of the studies there were some concerns about the risk of bias.
Publication bias
The result of Egger’s test revealed no substantial risk of publication bias neither for the intervention effect outcomes, nor for the maintenance ones (p-value > 0.1).
link







